FLAVOR CHOICE IN BOWEL PREPARATION

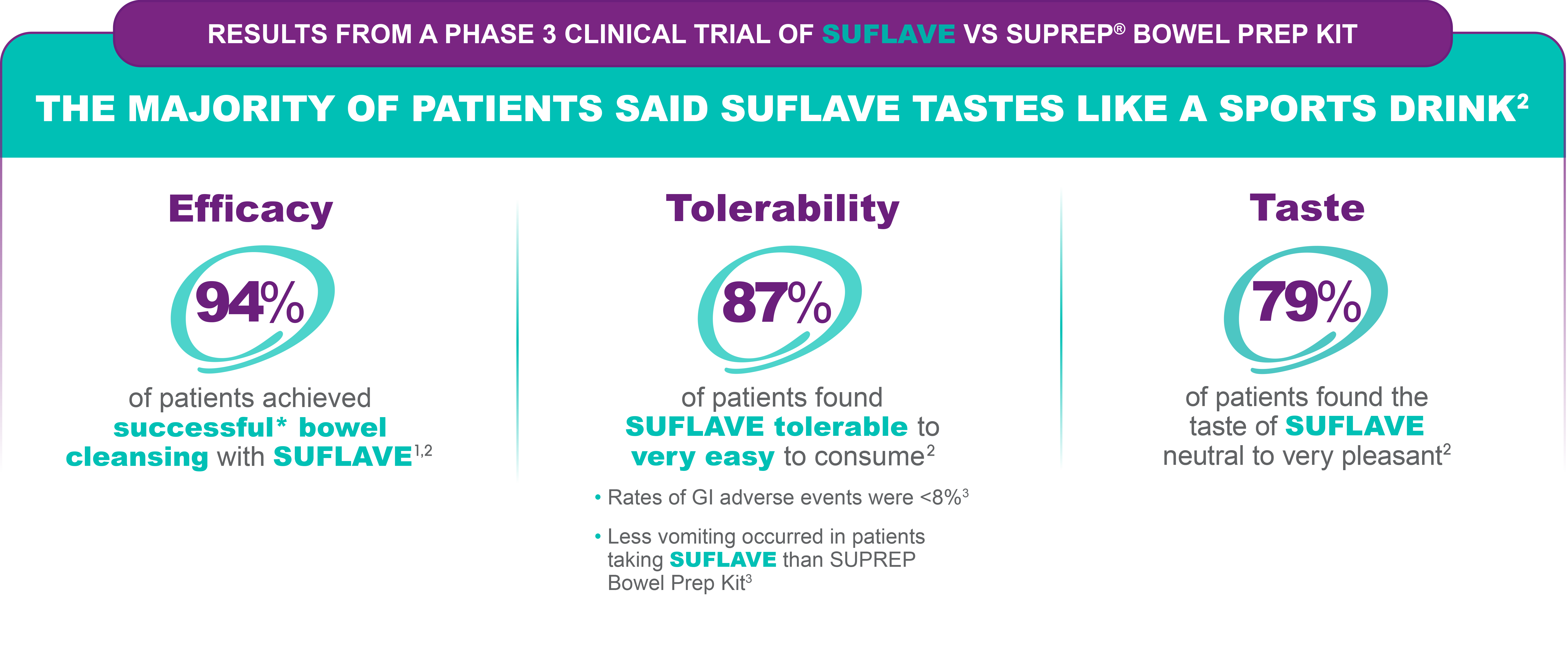

Study Design1,2: This phase 3 trial was conducted in multiple sites. Of the 500 subjects who enrolled, 450 were evaluable for efficacy analyses. The primary endpoint was the percentage of subjects with successful cleansing, which was based on the US FDA Bowel Prep Scoring Scale. The goal of the study was to establish non-inferiority of SUFLAVE™ to SUPREP® Bowel Prep Kit, using a 10% non-inferiority margin.
P<0.001 in this non-inferiority clinical trial.
Corporate Partnership
Braintree, a part of Sebela Pharmaceuticals®, is a proud supporter of the following organizations:



INDICATION
SUFLAVE™ (polyethylene glycol 3350, sodium sulfate, potassium chloride, magnesium sulfate, and sodium chloride for oral solution) is an osmotic laxative indicated for cleansing
of the colon in preparation for colonoscopy in adults.
DOSAGE AND ADMINISTRATION
A low residue breakfast may be consumed on the day before colonoscopy, followed by clear liquids up to 2 hours prior to colonoscopy. Administration of two doses of SUFLAVE™ are
required for a complete preparation for colonoscopy. Each bottle must be reconstituted with water before ingestion. Each bottle and one flavor enhancing packet are equivalent to
one dose. An additional 16 ounces of water must be consumed after each dose. Stop consumption of all fluids at least 2 hours before the colonoscopy.
CONTRAINDICATIONS
Use is contraindicated in the following conditions: gastrointestinal obstruction or ileus, bowel perforation, toxic colitis or toxic megacolon, gastric retention, hypersensitivity to any
ingredient in SUFLAVE™.
WARNINGS AND PRECAUTIONS
Risk of fluid and electrolyte abnormalities: Encourage adequate hydration, assess concurrent medications and consider laboratory assessments prior to and after each use;
Cardiac arrhythmias: Consider pre-dose and post-colonoscopy ECGs in patients at increased risk; Seizures: Use caution in patients with a history of seizures and patients at
increased risk of seizures, including medications that lower the seizure threshold; Colonic mucosal ulcerations: Consider potential for mucosal ulcerations when interpreting
colonoscopy findings in patients with known or suspected inflammatory bowel disease; Patients with renal impairment or taking concomitant medications that affect renal function:
Use caution, ensure adequate hydration and consider laboratory testing; Suspected GI obstruction or perforation: Rule out the diagnosis before administration; Patients at risk for aspiration: Observe during administration; Hypersensitivity reactions, including anaphylaxis: Inform patients to seek immediate medical care if symptoms occur.
ADVERSE REACTIONS
Most common adverse reactions (≥ 2%) are: nausea, abdominal distension, vomiting, abdominal pain, and headache.
DRUG INTERACTIONS
Drugs that increase risk of fluid and electrolyte imbalance.
View the Full Prescribing Information and Medication Guide.
References
1. SUFLAVE™ [package insert]. Braintree, MA: Braintree Laboratories, Inc.
2. Bhandari R, Goldstein M, Mishkin DS, et al. Comparison of a novel,
SUTAB® (sodium sulfate, magnesium sulfate, potassium chloride) tablets for oral use is an osmotic laxative indicated for cleansing of the colon in preparation for colonoscopy in adults.
CONTRAINDICATIONSUse is contraindicated in the following conditions: gastrointestinal obstruction or ileus, bowel perforation, toxic colitis or toxic megacolon, gastric retention, hypersensitivity to any ingredient in SUTAB®.
DOSAGE AND ADMINISTRATION
A low residue breakfast may be consumed. After breakfast, only clear liquids may be consumed until after the colonoscopy. Administration of two doses of SUTAB® (24 tablets) are required for a complete preparation for colonoscopy. Twelve (12) tablets are equivalent to one dose. Each SUTAB® bottle contains a desiccant. Remove and discard the desiccant from both bottles the evening prior to the colonoscopy. Water must be consumed with each dose of SUTAB® and additional water must be consumed after each dose. Complete all SUTAB® tablets and required water at least 2 hours before colonoscopy.
WARNINGS AND PRECAUTIONS
Risk of fluid and electrolyte abnormalities: Encourage adequate hydration, assess concurrent medications and consider laboratory assessments prior to and after each use; Cardiac arrhythmias: Consider pre-dose and post-colonoscopy ECGs in patients at increased risk; Seizures: Use caution in patients with a history of seizures and patients at increased risk of seizures, including medications that lower the seizure threshold; Patients with renal impairment or taking concomitant medications that affect renal function: Use caution, ensure adequate hydration and consider laboratory testing; Colonic mucosal ulcerations: Consider potential for mucosal ulcerations when interpreting colonoscopy findings in patients with known or suspected inflammatory bowel disease. Suspected GI obstruction or perforation: Rule out the diagnosis before administration. Hypersensitivity reactions, including anaphylaxis: Inform patients to seek immediate medical care if symptoms occur. Risk of Gastrointestinal Complications with Ingestion of Desiccant: Postmarketing reports of ingestion of the desiccant along with SUTAB® tablets has been reported and may be associated with risk of gastrointestinal complications and/or choking.
ADVERSE REACTIONS
Most common gastrointestinal adverse reactions are: nausea, abdominal distension, vomiting, and upper abdominal pain.
DRUG INTERACTIONS
Drugs that increase risk of fluid and electrolyte imbalance.
